

The effect of calcitonin upon the proliferation of giant cell tumor; Preliminary of 9 cases
Visit Rangsinaporn, M.D.* Thanya Subhadrabandhu, M.D.**
Patarawan Woratanarat, M.D.** Vorachai Sirikulchayanonta, M.D.***
* Department of Orthopaedics, Faculty of Madicine, Srinakarinwirot University, Thailand
**Department of Orthopaedics, Faculty of Madicine, Ramathibodi Hospital, Mahidol University, Thailand
***Department of Pathology, Faculty of Madicine, Ramathibodi Hospital, Mahidol University, Thailand
Abstract
Giant cell tumor is one of the most common primary bone tumors in adult. Current therapy is still curettage and bone graft packing with adjuvant chemical and thermal cautery. However, the rate of recurrence is rather high ranging from 20 to 85 % and many attempts have been made to decrease this rate. Some investigators showed that the cells of giant cell tumor share similarity to osteoclasts in terms of phenotypic expressions and calcitonin receptor. In addition, calcitonin was reported to cause regression and degeneration of this tumor. Our study is aimed to evaluate the effect of calcitonin upon this tumor by comparing the number of positive cells in PCNA staining between pre and post calcitonin administrations. The result revealed significant decrease in number of positive cells after calcitonin given with p<0.001
Introduction
Giant cell tumor is one of the most common primary bone tumors in adult. Giant cell tumor accounted for 5.12% of primary bone tumors and 22.7% of benign bone tumor [1]. Giant cell tumor at Ramathibodi Hospital, Thailand is 7% of primary bone tumors. It is the second most common bone tumor following osteosarcoma [2]. Current therapy is curettage and bone grafting with adjuvant therapy using chemical or thermal cautery. Even though these types of treatments yielded acceptable result, local recurrences were still a common problem, especially in grade 3 group ( Campanaci grading system ). Local recurrence rate in this grade 3 group was about 20-85%. Radiotherapy has favorable result, but there is a chance of malignant transformation to secondary sarcoma. To our knowledge, chemotherapy or newly developed therapy which can reduce local recurrent rate is still challenging. Calcitonin is peptide hormone, released from parafollicular C-cells of thyroid gland in hypocalcemic state, was known to inhibit bone resorption by inactivating osteoclast and make cell morphologic change and result in loss of cell mobility [3,4,5]. It is our aim to study the effect of calcitonin upon giant cell tumors by using technique of PCNA staining to compare the proliferative activity of cells in giant cell tumor before and after calcitonin treatment.
Meterials and Methods
All cases of giant cell tumor patients at Ramathibodi Hospital during May 1st 2000 and January 30th 2002 were included in this study. The study was approved by hospital ethical committee. All cases were biopsied by our senior orthopaedist and histopathological diagnosis was done by our senior orthopaedic pathologist. After the diagnosis of giant cell tumors was made, patients were given a daily dose of synthetic salmon calcitonin (MiacalcicR ) 100 IU subcutaneously for 14 days. After finishing 14 days of calcitonin administration, patients were performed definitive surgery by the same senior orthopaedist. Types of operation were depend on tumor stagings. The surgical specimens which obtained from first and second operations were submitted to the same pathologist for pathological diagnosis. Immunoperoxidase stainings by using monoclonal antibody PCNA (Immunotech) were performed. The nuclear stainings of epithelial cells of colonic mucosa were used as control. Ten high power fields (40x ) per each slide were randomized, captured and saved by using software Olympus CW 95. Countings of the staining cells were performed by the same investigator and used Soft ware Image Pro Plus which can mark cells that have been counted ( Fig. 1). Cell counting was done by one investigator, whom was blinded for clinical information in every specimen. The measurements for each group of cells were expressed by mean +SD. Comparing proliferative activity of cells between before and after calcitonin administration was performed by using paired t-test
RESULTS
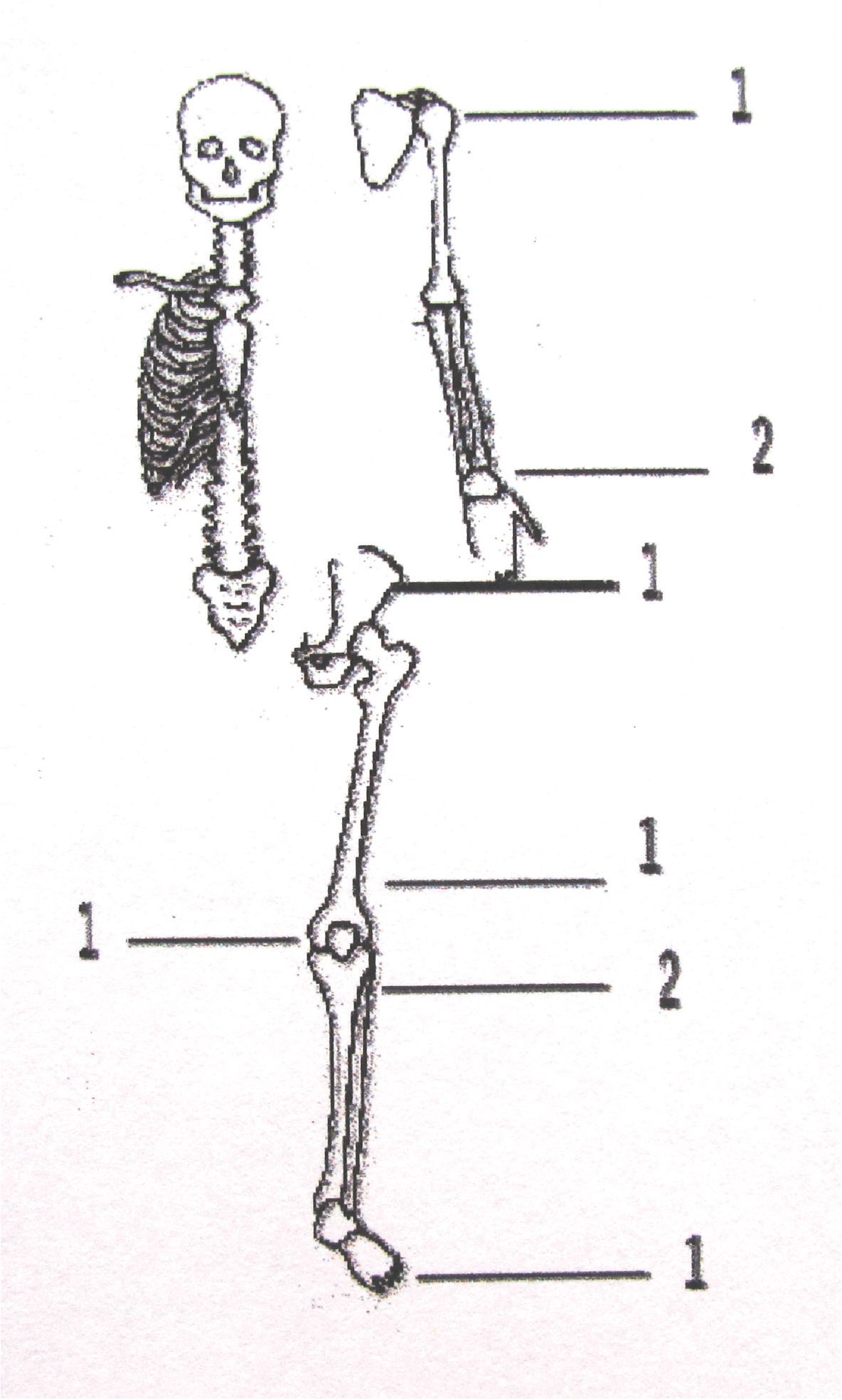
There are 4 male and 5 female were included in this study, total number were 9 patients. Mean age was 25 years, ranged 18-24 years. Tumor locations were shown in Fig. 2. Number of stained positive mononuclear spindle cells decreases significantly after calcitonin administration in the same patient (P-value 0.05). Ratio of stained positive cells to total cells decreases without statistically significant after calcitonin administration. Total number of tumor cell decreases without statistic significant after calcitonin administration. Number of stained positive Giant cell group can not be evaluated due to very little number of staining cell.
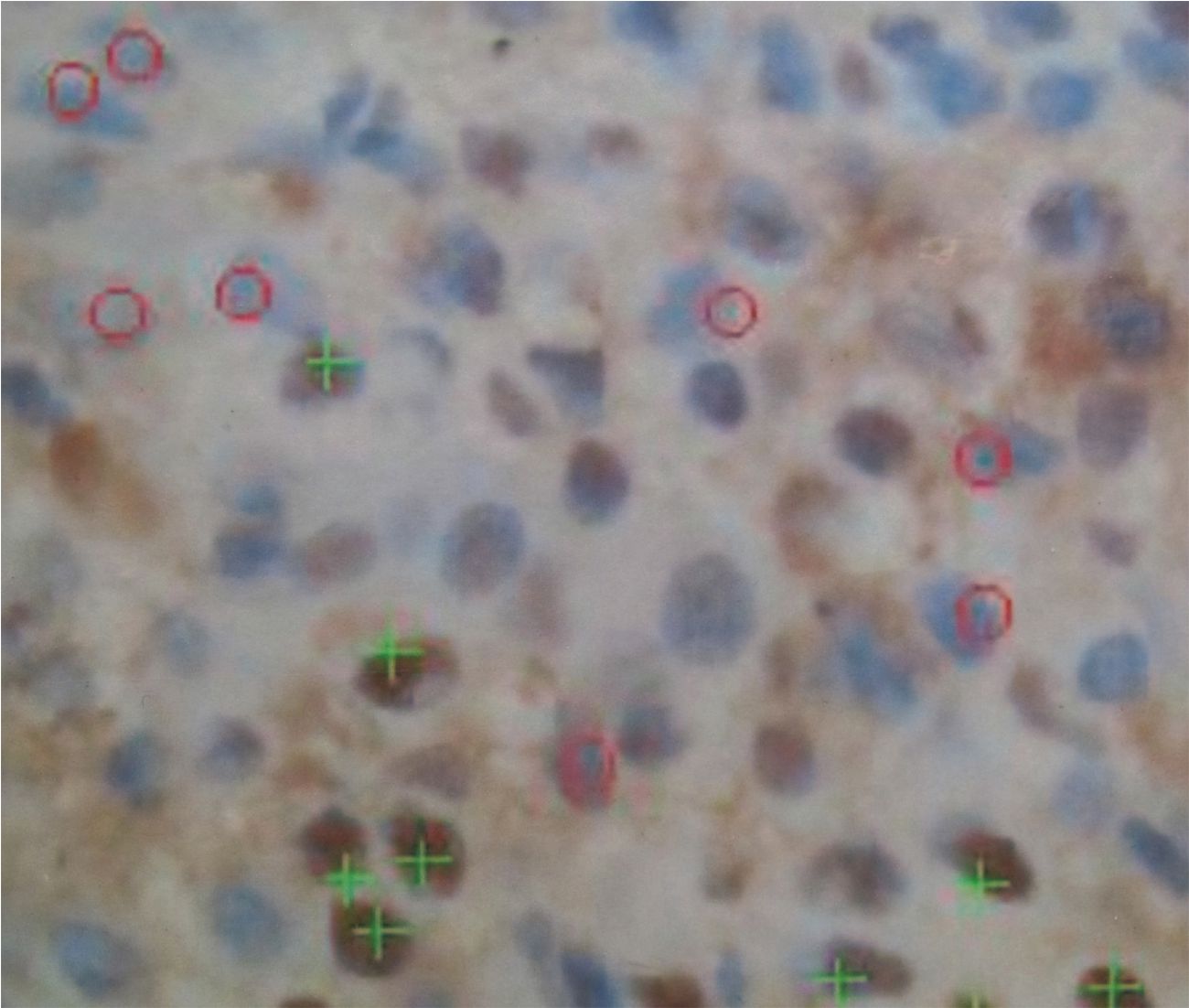
Fig. 1 showing marker while using program Image Pro Plus to count stained positive and negative mononuclear spindle cell
(pre calcitonin)
Fig. 2 showing location of tumor in 9 patients
Table 1 showing demographic data and cell counting results
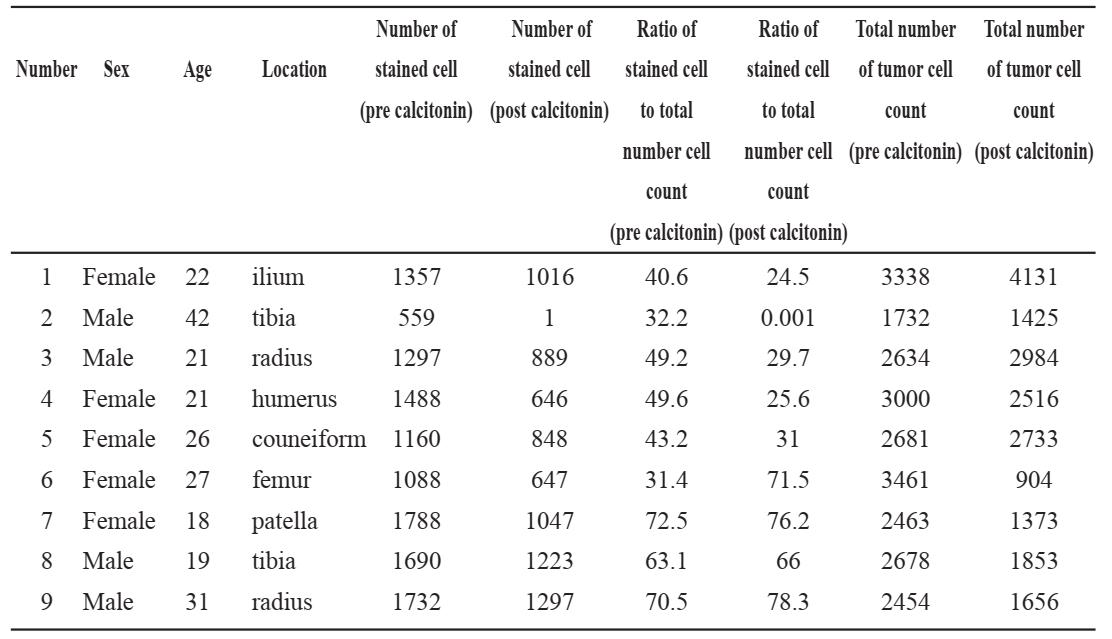
Table 2 showing means of number of positively stained mononuclear spindle cells before and after calcitonin administration Spindle cell
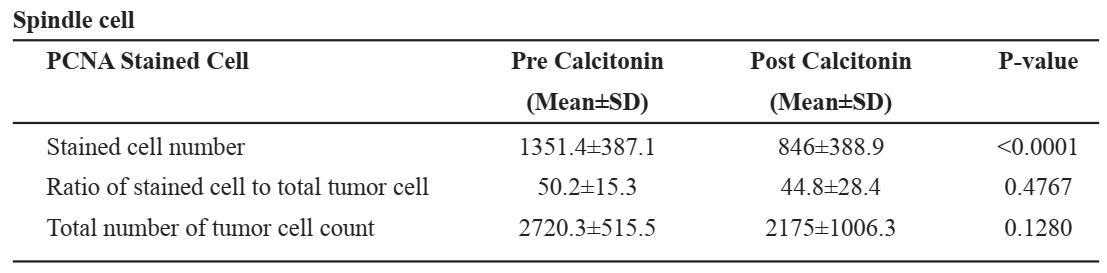
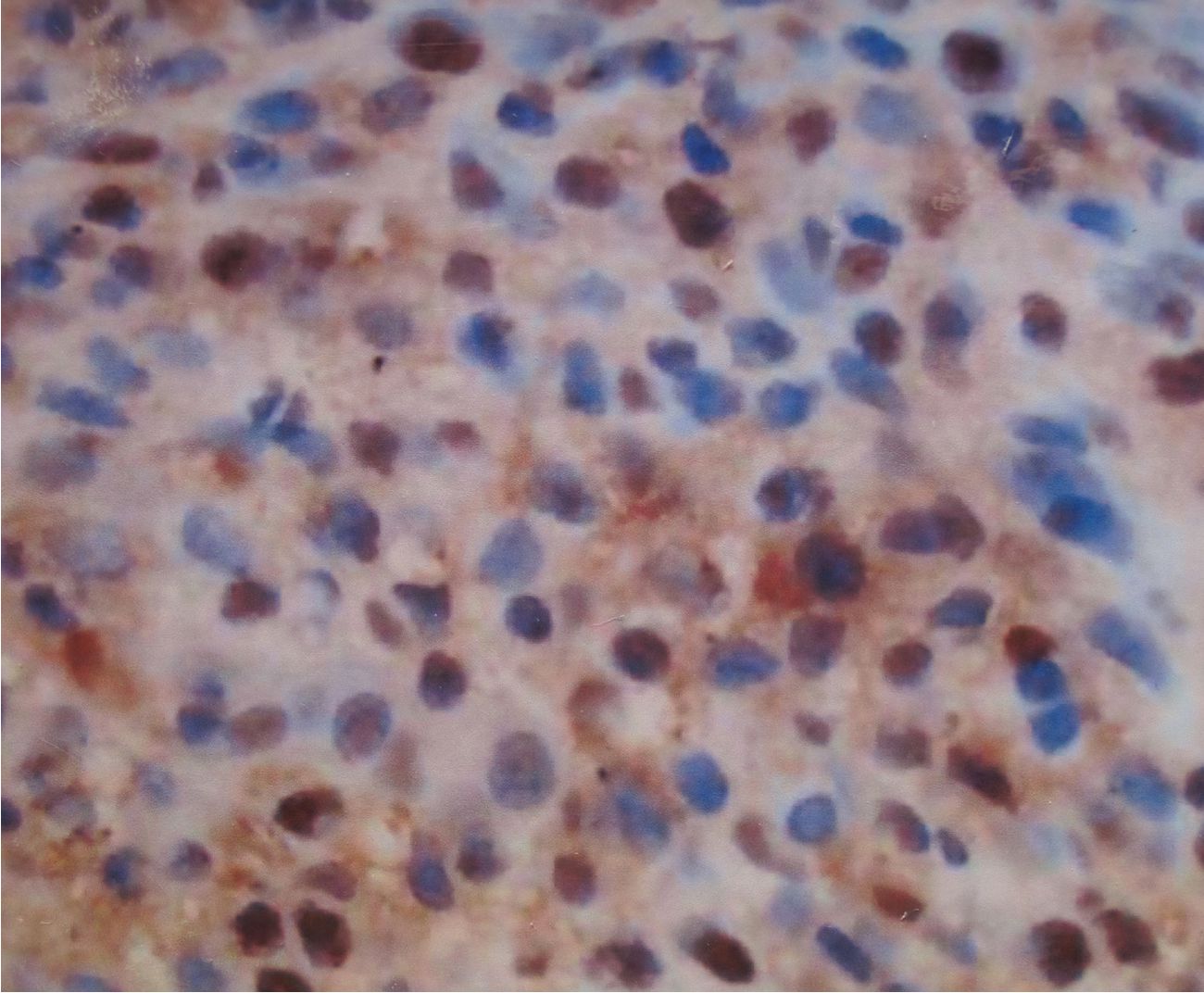
Fig. 3 showing PCNA stained cell before calcitonin administration
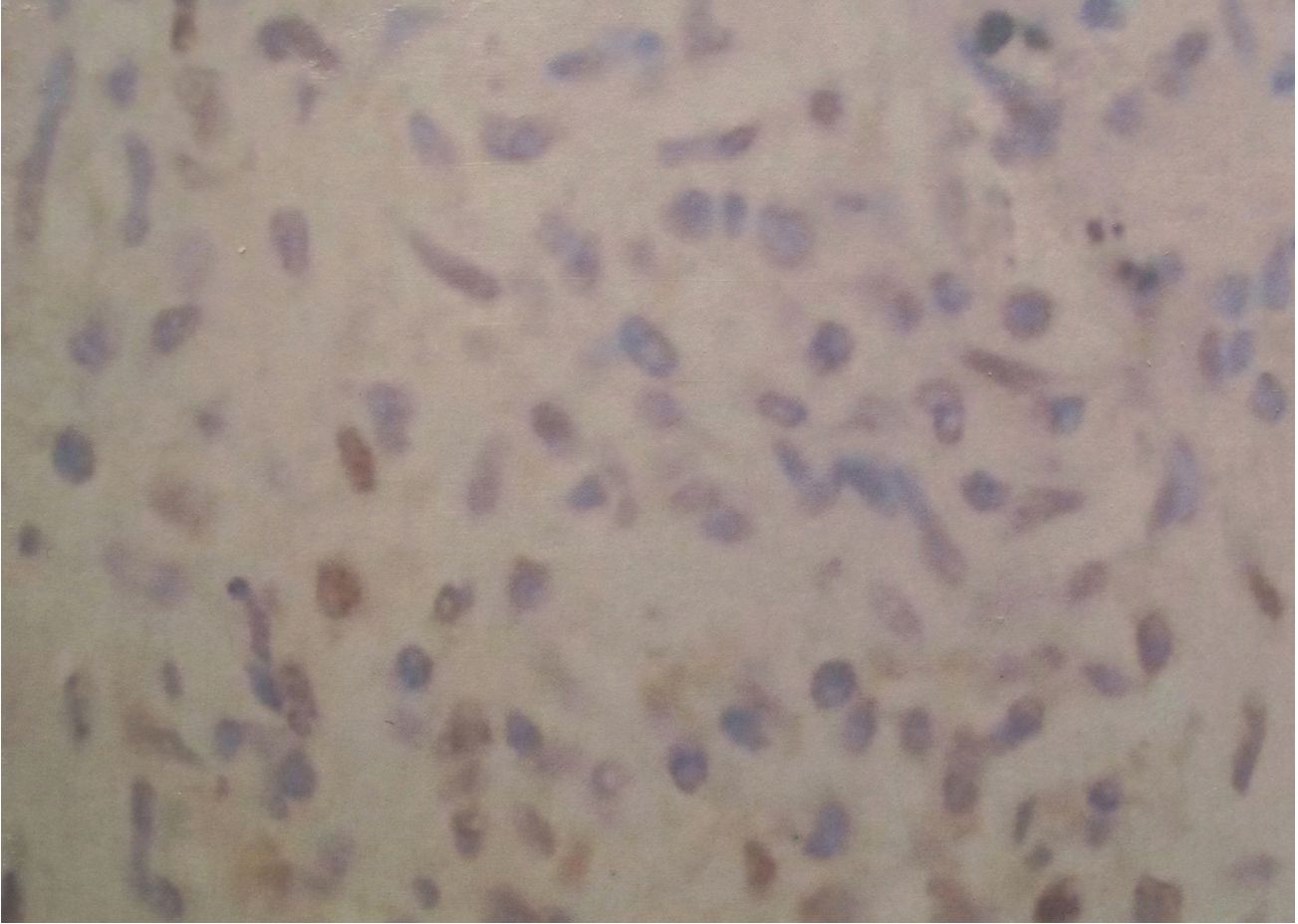
Fig. 4 showing PCNA stained cell after calcitonin administration in the same patient
DISCUSSION
Giant cell tumor are composes of three different cell types , multinucleated giant cell, mononuclear round cell and mononuclear spindle cell. The multinucleated giant cell has calcitonin receptor but does not have monocyte-macrophage surface antigen , which is phenotype marker of osteoclast. From his-tochemical study found that both histochemical behavior and physiologic behavior of multinucleated giant cell of giant cell tumor and osteoclast are the same. The mononuclear round cell shows monocyte macrophage (histiocyte marker). The most important cell type for this paper is mononuclear spindle cell. The mononuclear spindle cell represents neoplastic proliferation of tumor. Its phenotypic characteristics resembles connective tissue stroma cell. It does not have macrophage surface antigen but it has receptor for parathyroid hormone. Willing M et al [6] found that stromal cell stimulates blood monocyte migration in tumor tissue and helps in cell fusion to form osteoclast-like multinucleated giant cell. The osteoclast-like multinucleated giant cell has similar function to osteoclast in bone resorption and osteolysis . Calcitonin is peptide hormone, released from parafollicular C-cells of thyroid gland in hypocalcemic state [3,4]. Calcitonin inhibits bone resorption by inactivate osteoclast and make cell morphologic change and result in loss of cell mobility. (14) Iida et al [7] found that human and salmon calcitonins have the same inhibitory effect on bone resorbing activity. They used cells in giant cell tumor of bone instead of osteoclasts to study in human bone resorbing activity. They found that tumor cells showed loss of bone resorptive function after calcitonin was administered in cultured cells. Synthetic salmon calcitonin was commonly used in treatment of osteoporosis by means of inhibiting osteoclast activity [8] . Umeda et al [9] reported of calcitonin administration for treatment of giant cell tumor of the bone in human. They found that calcitonin cause tumor regression and degenerative necrosis.
Komiya et al [10] found that mononuclear cell shows phenotypic characteristic of both osteoclast and monocyte-macrophage and it also has calcitonin receptor. Meada et al [11] showed that neoplastic mononuclear spindle cell contain saturable, specific, highly-affinity calcitonin receptor and calcitonin administration can change cell morphological and physiological function of cell. Calcitonin affects cell by inhibiting DNA synthesis. Oreffo et al [12] found that mononuclear cells of giant cell tumor have phenotypic characteristic closer to osteoclast than macrophage. These cells response to osteotropic factors such as 1,25 dihydroxy vitamin D3 and insulin-like growth factor and can produce soluble factor stimulating osteoclastic bone resorption. Lau et al [13] showed that mononuclear and giant all components of giant cell tumor have similar phenotypic features of osteoclast and stimulate osteoclast formation and resorption Proliferating Cell Nuclear Antigen (PCNA) is a group of protein which accumulated in interphase stage of cell cycle and disappeared in the end of mitosis stage. PCNA is found in DNA polymerase and it is important for completion of cell cycle[14]. Paulo et al [15] used PCNA staining for evaluating cell activity of giant cell tumor and found that PCNA staining can show tumor cell activity . Tumor cell activity can be measured by counting stained positive cells, which represent cell proliferation.
This study used subcutaneous injected calcitonin instead of nasal inhalation calcitonin in order to give the effective dose of calcitonin. Duration of calcitonin injection is 14 day, which should not delay definitive surgery. Route administration , dose and duration of calcitonin administration should be adjusted in the future study in order to achieve more accurate result. All patients should be followed for more longer period to evaluate local recurrence. Result of this study shows that stained positive mononuclear spindle cell number decrease significantly after calcitonin administration similar to that of Iida and Umeda studies [7,9 ]. These revealed that calcitonin can inhibit activity of spindle cell of giant cell tumor. Our result showed that ratio of stained positive spindle cell per total cell decreased after calcitonin administration without statistical significant and total tumor cell number decrease without statistical significance and this may be explained by the hypothesis that all tumor cell does not have calcitonin receptor. Noari et al [16] reported using calcitonin as adjunct therapy after curettage in 25 patients. They reported local recurrence rate 52% after 68 month of follow up. They concluded that using calcitonin as adjuvant for surgery is not effective to decrease recurrent rate. But the dose and duration of calcitonin administration should be adjusted to improve effectiveness of treatment
This study is a pilot study and requires further study with increasing more patients. It also requires a longer period of time of follow-up to evaluate tumor local recurrent rate after treatment. However this study clearly showed that mainly spindle tumor cells were affected and decreased proliferation after calcatonin administration, which corresponded with our proposed hypothesis.
REFERENCE
1. Dahlin DC Unni KK; Giant cell tumor (Osteoclastoma). In Dahlin’s Bone Tumors General Aspects and Data on 11,087 case, 5th Edition, Lippincott-Raven Publisher, Philadelphia, 1996: 263-84.
2. วรชัย ศิริกุลชยานนท์. (2540) เนื้องอกชนิด Giant cell tumor. ใน เนื้องอกของกระดูก (พิมพ์ครั้งที่ 2). เจ.ฟิล์ม โปรเซส จำากัด.กรุงเทพมหานคร. หน้า 108-117.
3. Steven R. Goldring. M.D. .Alan L. Schiller, M.D., Henry J. Mankin, M.D., Jean-Michel Dayer. M.D., and Stephen M. Krane. M.D. Characterization of cells from human giant cell tumor of bone. Clin Orthop 1986; 204 : 59.
4. Foster GV, Baghdianz A, Kumar MA, Slack E, Soliman HA, MacIntyre I Thyriod origin of calcitonin. Nature 1964; 202:1303-305.
5. Chambers TJ, Chambers JC, Symonds J, Darby JA . The effect of human calcitonin on the cytoplasmic spreading of rat osteoclasts. J Clin Endocrinol Metab; 63:1080-85.
6. Willing M, Engels C,Jesse N,Werner M, Del-ling G,Kaiser E . The nature of giant cell tumor of bone. J Cancer Res Clin Oncol 2001; 127(8):467-74
7. S. Iida, S. Kakaudo, Y. Mori, M. Matsui, K magota, Y. Kitajima, N. Nakamura, K. Mano, Y. Hakada, H. Azuma, T. Kurokawa, M. Ku-megawa : Human calcitonin has the same inhibitory effect on osteoclastic bone resorption by human giant cell tumor cells as salmon calcitonin. Calcif Tissue Int 1996;59 : 100-4.
8. Azria M ; Calcitonin in therapeutic use. In The Calcitonin Physiology and Pharmacology. S. Karger AG, Basel, 1989:1933-44
9. Umeda T, Kuwabara T, Takada N : Clinical application of calcitonin for giant cell tumor of bone (in Japanese). Jpn J Cancer Chemother 1988 ; 15 : 356-7.
10. Komiya S, Sasaguri Y, Inoue A, et al : Characterization of cells cultures from human giant cell tumors of bone. Clin Orthop 1990; 258:304-9
11. Akio Maeda, Hisao Matsui, Masahiko Kan-amori, Kazuo Yudoh, Haruo TsuJi . Calcitonin receptors on neoplastic mononuclear cells cultured from a human giant cell tumor of the sacrum. Clin Oncol 1994; 120:272-8.
12. Oreffo R, Marshall J, Kirchen M et al : Characterization of a cell line derived from a human giant cell tumor that stimulate osteoclastic bone resorption. CORR 1993; 269:229-241
13. Lau YS, Sabokbar A, Gibous CL, Giele H, Athanasow N. Phenotypic and molecular studies of giant cell tumor of bone and soft tissue. Hum Pathol. 2005; 36 (9) : 945 - 54
14. P A Hall,D A Lavinsor: Review. Assessment of cell proliferation in histological material. J Clin Pathol 1990; 43 : 184-92.
15. Paulo E, Julia F, Junia N, Ricardo S. Immunohis-tochemical expression of p53,MDM2,Ki67and PCNA in central giant cell granuloma and giant cell tumor : J Oral Pathol Med 1999; 28:54-8
16. Nouri H, Hedi Meherzi M, Ouertatani M, Zehi K, Douik M, Zouari M. Calcitonin use in giant cell bone tumors. Orthop Traumotol Surg Res . 2011; 97 (5) : 520 - 6 . Epub 2011 Jun 30